
By Belinda Castles
Researcher | Kairangahau
Skin cancer is the most common cancer in New Zealand – but it’s also one of the most treatable if caught early. From checking your own skin to seeing a GP, using mole-mapping services or trying smartphone apps, there’s no shortage of ways to spot potential problems.
But how reliable are these options? And when should you use them?
We asked six experts about the different detection methods – and what you need to know before relying on them.

Should I self-check for skin cancer?
In the past 12 months, according to the 2025 SunSmart in Aotearoa New Zealand Survey, 26.8% of New Zealanders conducted a skin check themselves or had someone who wasn’t a medical professional do it for them.
All the experts we spoke to emphasised the importance of checking your skin regularly for changes.
Melanoma NZ’s chief executive, Andrea Newland, said research suggests most melanomas are first recognised by the person themselves or a family member. Early detection through self-examination potentially reduces the risk of advanced melanoma by 63%.
Amanda Dodd, the Cancer Society of New Zealand’s advocacy and public affairs lead, said it’s important to check over your entire body regularly – at least monthly. Skin cancers can be in places you can’t see yourself, so it’s a good idea to ask someone to help you check. If you don’t have someone to help you check difficult-to-see places, try using a hand mirror.
“Check your armpits, behind your ears, your scalp, your bottom, the bottom of your feet, palms of your hands and your nails. Seek medical advice if you notice a spot or mole that’s new or has changed. This could include a change in colour, shape or size or if you have a sore that doesn’t heal, is itchy, swelling or bleeding.”
General surgeon and chair of Skin Cancer NZ, Dr Susan Seifried, said you also need to be aware that not all melanomas will be brown or black. Some melanomas can look similar to non-melanoma skin cancer – pale pink or more purple/red and may be quite flat and not “bad looking” in the early stages.
Use the alphabet to check spots
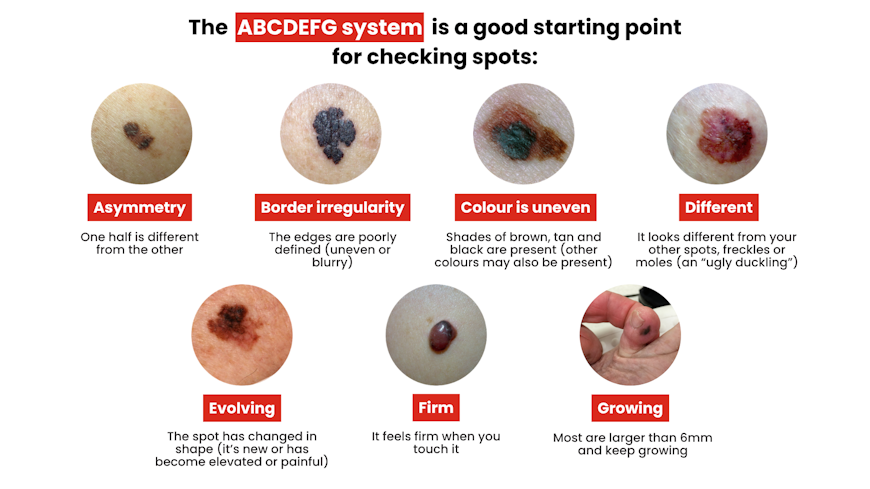
These images are indicative only. Look for the type of behaviour described, rather than trying to match your lesion to the image.
Source: Melanoma New Zealand.
Do skin-checking smartphone apps work?
With a skin cancer app, you can use your smartphone to take a photo of a mole or lesion and get an assessment of its risk.
You’ll usually also be asked to give a patient history, including a history of skin cancer and the number of moles you have.
There are two main types of app.
Teledermatology or doctor report apps give you a risk classification based on the photo you send to a skin specialist. An example of this type of app would be First Derm.
Algorithm apps use a mathematical process to analyse the photo and provide a risk classification. SkinVision is one such app.
While the apps are usually free to download, you’ll pay for their services. SkinVision costs around $14 per check or $50–$100 for a subscription. First Derm is typically $40–$110 per consultation, depending on how quickly you want a response. Be aware that First Derm’s dermatologists are not registered or based in New Zealand.
Andrea Newland said apps shouldn’t be seen as a substitute for a face-to-face consult or a full-body check. She said AI and automated diagnostic tools are increasingly being incorporated into skin-imaging technologies but are best used in the hands of trained health professionals.
Dermatologist Amanda Oakley agreed.
“They do have a place in tracking skin lesions. But it’s important anything changing, bleeding, crusted or abnormal is checked by a GP.”
Dermatologist Dr Monique Mackenzie (Ngāti Tūwharetoa) cautions that algorithm-based diagnostic apps are not trained using enough or any Pacific or Indigenous skin types, particularly in the skin cancer setting. This means their diagnostic accuracy is unknown for these skin types.
Other concerns raised about the apps include that people will only take a photo of moles they can see, and there is the potential for incorrect results, which can give a false sense of security or generate unnecessary anxiety.
The Cancer Society has also cautioned against relying on apps to detect skin cancer.
Do I need an expensive skin cancer check?

Some companies offer skin checking or surveillance services, commonly referred to as “mole mapping”. These services use a combination of detection techniques, including dermoscopy (magnified images using a tool called a dermatoscope), total body photography, AI technology and health professional diagnosis.
Examples of these services include Molemap, where a full skin exam costs $399, and Molecheck, where a full skin exam will set you back $325.
Katrina Patterson, chief executive of Skin Cancer NZ, said these services can be valuable for those at high risk of skin cancer as they’re useful for tracking lesions. However, she cautioned they can be expensive.
“GPs and nurses with early detection training can also provide thorough skin checks with lesion photography at a lower cost,” she explained.
Amanda Oakley said the follow-up checks with dermoscopy, compared with previous photographs, can detect changing lesions before they can be reliably diagnosed with the naked eye.
Before paying for one of these services, the Cancer Society recommends you consider the following issues.
What services are offered – a total body examination or only a check of certain lesions?
What level of training has the provider undertaken?
What will it cost? Is there a cost beyond the initial consultation, such as a charge for storing images or extra costs for follow-up visits?
What follow-up is provided? Will results be shared with your GP?
Can my GP check me for skin cancer?
GPs are often the starting point for people wanting a skin check. This is particularly the case in regional areas that don’t have other skin checking options.
Susan Seifried said you should visit your GP as soon as you notice anything suspicious on your skin.
“The sooner it’s removed, the more superficial it is and the more likely you’ll only need a simple operation to treat it. In some cases, you won’t even need an operation – early forms of skin change can be treated with topical ointments.”
Amanda Oakley said while health professional scarcity and training are a challenge for skin cancer detection, she’s excited progress is being made.
“Skin Cancer New Zealand is developing a comprehensive online skin cancer and dermoscopy course. With support from Health New Zealand, it will be available to health professionals later this year.”
GPs are responsible for about 80% of skin removals. Oakley said a trained, experienced doctor will remove up to five harmless lesions for every melanoma. But a less trained and experienced doctor might remove far more “to be safe”.
When lesions are uncertain or more difficult to manage, GPs will refer patients to either a dermatologist or a public hospital. If you have health insurance, you may be referred to a private provider. Some insurers will cover you to see a private skin cancer specialist or private dermatologist without a referral.

Compare health insurance policies
Use our interactive database to compare health insurance cover and benefits for the policies in our survey.
How can I prevent skin cancer?
Amanda Dodd said early detection goes hand in hand with prevention.
“Around 90% of skin cancers are preventable. The steps we take, like covering up, spending time in the shade, using sunscreen and avoiding sunbeds, are simple but important measures.”
Despite this, Dodd said many New Zealanders still regularly get sunburnt, and young adults are vulnerable to pro-tanning messages that put them at higher risk.
“I would love to see sun protection as routine as brushing your teeth. That would help people feel in control of their skin health rather than fearful of it.”
Susan Seifried said she wishes more people knew that skin cancer is preventable.
“Our melanoma death rate is similar to the road toll but is much easier to prevent. We need to build a culture of sun-smart behaviours and mandate sun protection policies in schools, workplaces and other community settings.”
Seifried said sun exposure in people under the age of 30 is highly predictive of future skin cancer.
“Many of my older patients mourn the fact ‘no one knew’. We don’t have that excuse today, and we need to do better.”
For tips on how to stay safe in the sun, visit our sun protection hub.
Three real-life skin cancer stories
Tony
“I’m a walking surgical example of why you should get your skin checked frequently.
I had my first melanoma removed in 2001. It was a small lump on my skull, and my GP decided to chop it out. It was cancerous, and that was the start of my skin cancer journey. For me, 6-monthly skin checks are essential, and over the last few years, I’ve had about a dozen skin cancers removed.”
Margaret (Ngāti Kuri/Ngāti Porou/Te Aitanga a Hauiti) highlighted the importance of skin checks irrespective of skin colour.
“I had a spot on my nose for about 10 years that would sometimes bleed. Eventually, I made an appointment with a skin-screening company. The report recommended the spot be removed – biopsy results confirmed it was a basal cell carcinoma.”
Ron
“I delayed getting a spot checked on the top of my head. When it was finally removed, the biopsy showed further surgery was required to remove a larger amount of tissue, which required a skin graft from my thigh.
“As a result of my tardiness, I now have a large crater on the top of my head. Mercifully, it was not melanoma, but an earlier diagnosis may have avoided the procedures I went through. I hope my case encourages others to seek more urgent advice.”
Many people also contacted us about the importance of being vigilant when a spot looks suspicious. Thanks to everyone who shared their stories.
Am I at risk of skin cancer?
Skin cancer – the uncontrolled growth of abnormal skin cells – is the most common cancer affecting New Zealanders. In 2025, the cost of skin cancer to the New Zealand health system was estimated to be more than $455 million.
There are two main classifications of skin cancer.
Melanoma is the most serious. If left untreated, it can spread quickly and be fatal. New Zealand has the highest death rate from melanoma in the world. According to Melanoma New Zealand, every year more than 8,000 melanomas are diagnosed in this country and almost 300 New Zealanders die from melanoma.
Non-melanoma skin cancer refers to all other types of skin cancer. The most common are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). BCCs are the most common and tend to grow slowly. SCCs are more aggressive than BCCs and are responsible for most non-melanoma skin cancer deaths. Exact figures are unknown (new cases aren’t registered), but it’s estimated 90,000 New Zealanders are treated for non-melanoma skin cancer each year.
Skin cancer rates are highest among fair-skinned New Zealanders. However, when diagnosed, Māori are 2.6 times more likely to die from a skin cancer than non-Māori – the largest survival disparity between Māori and non-Māori of any cancer.
Katrina Patterson chief executive of Skin Cancer NZ said Māori are more likely to be diagnosed later, which leads to poorer survival rates.
“Māori, as well as Pacific and Asian people, don’t often display the typical characteristics associated with melanoma risk, such as fair skin, freckles and red or blonde hair. But they often have thicker, more serious melanomas once detected.”
Monique Mackenzie said there’s a persistent misperception both in the community and amongst some health professionals that if you have olive or darker skin, you are not at risk of developing skin cancer.
“This is simply not true, and quite a harmful misconception. There is consistent research showing Māori and Pacific people not only develop skin cancer but also have a higher portion of high-risk melanoma.”
You are also at increased risk if you have:
a family history of skin cancer
skin damage due to sunburn
used a sunbed
many and larger moles
a weakened immune system.
Health New Zealand | Te Whatu Ora funded this article as part of its ongoing efforts to raise awareness about sun protection and skin cancer risks.



